Digoxin and Ferusemide in Enteral Feeding
This content was published in 2000. We do not recommend that you take any clinical decisions based on this information without first ensuring you have checked the latest guidance.
Nutritional status is now recognised to be an important part of medical care and nutritional support can be provided enterally or parenterally in various patient groups. Both routes may be used for short term feeding in the acute setting or long term in the community. Patients with Crohn's disease are an example of those who may need long term total parenteral nutrition (TPN).1
The use of either the enteral or parenteral route provides pharmaceutical challenges in the delivery of medication usually delivered by the oral route.
This article discusses how these challenges may be approached.
Details of the general effects of nutritional status on drugs are beyond the scope of this article, but factors such as concomitant disease states (renal failure, hepatic failure, short bowel syndrome), obesity or malnutrition can alter the pharmacokinetics or bioavailability of a medicine. Drug effects such as drug-induced folate or vitamin B6 deficiency, drug-induced electrolyte imbalances, or effects of electrolyte imbalances on drugs, such as lithium may also need consideration. General mechanisms of interactions between drugs and nutrients may include stimulation of blood flow to the splanchnic capillary network (increasing absorption), chelation of drug molecules by minerals such as calcium and iron, competing with the action of the drug (for example, vitamin K and warfarin), changing the pH of the gastrointestinal (GI) tract to increase or decrease absorption, blocking or enhancing metabolism and causing changes in gut motility to increase or decrease absorption.2,3
Background
In a study of all drug-related problems in 440 clinical nutrition patients, the most frequent problems related to drug interactions or incompatibilities with enteral or parenteral nutrition, and inappropriate administration techniques.4
The nursing profession has demonstrated a significant interest in this issue and this is reflected in the numerous publications discussing drug administration, particularly in enterally fed patients, and frequent requests for advice on this subject from pharmacy staff. Despite this interest, several surveys have highlighted deficiencies in knowledge among nursing staff who routinely give drugs via a nasogastric (NG) tube, and practice has often developed by "trial and error". Naysmith and Nicholson found that the majority of nurses surveyed were unaware of issues involved in giving a sustained release preparation of theophylline, few knew to stop feeds before and after giving NG phenytoin, and there was great variation in the volumes of diluent used to flush drugs down NG tubes.5
In a survey carried out in the USA, 74 per cent of critical care nurse respondents used two or more inappropriate administration techniques for administering medications. Those who consulted pharmacy staff were more likely to use appropriate formulations and reported less obstructions of feeding tubes. However, only 6.2 per cent of respondents listed pharmacists as their primary source of knowledge.6 The authors of these studies concluded that lack of information contributed to the problems with administering drugs to patients on feeding tubes, and suggested that practice could be improved by involvement of pharmacists in establishing guidelines and training nurses. Pharmacists are ideally placed to liaise with other members of multi-disciplinary teams such as dieticians, speech therapists, and medical and nursing staff, to identify and address pharmaceutical problems in this group of patients (see Panel 1).
More recently, a pharmaceutical needs assessment of patients using enteral feeding tubes in the community covered by the Greater Glasgow health board confirmed that pharmacists need to be more actively involved in the medicines management of these patients, and better communication was required between primary and secondary care.
Pharmacists could provide advice on the availability of suitable preparations for enteral administration, drug-feed interactions and incompatibilities.7
Drug incompatibilities and interactions may also occur in patients receiving TPN. For example, warfarin resistance has been reported in patients receiving lipid TPN.8 Although mixing drugs with TPN or administering drugs and TPN through the same line is not recommended, in practice there may be occasions when there are no alternatives.
Panel 1: Possible roles for pharmacists managing patients on artificial nutrition
1. Advising on suitable routes of drug administration, formulation or alternative preparations
2. Advising on medication timing and alerting nursing staff to drugs which may have to be given outside routine drug rounds
3. Monitoring for loss of efficacy or toxicity due to drug interactions with feeds and reduced absorption owing to feeding tube site, etc
4. Educating nursing staff about administration techniques and contributing to in-service training
5. Liaising with the multi-disciplinary team to identify patients requiring pharmacist input; producing local guidelines; auditing of administration techniques
6. Discharge planning: liaison between hospital and community pharmacies over formulations, etc; educating patient or carer about appropriate administration techniques; providing back-up information
Searching for a route
In all patients who are unable to take oral medication, the pharmacist should review the need for medication before searching for an alternative route. This includes those prescribed enteral or parenteral nutrition.
In the acute situation, when patients are very unwell or peri-operatively, previous medication may no longer be appropriate, both temporarily and long term. For example, warfarin may sometimes be discontinued or substituted temporarily with intravenous heparin therapy.
Lithium therapy, hormone replacement therapy and monoamine oxidase inhibitors (MAOIs) are usually stopped peri-operatively and this avoids problems with administration.9
Sometimes drugs may be suspended for short periods without causing significant harm to the patient, as in statin therapy. If, however, drugs are considered necessary, but no other route is available, the reasons for a "nil-by-mouth" order and the possibility of enteral administration should be discussed with clinicians.
Where there is a need for medication, consideration should be given to the alternative routes available before choosing a preparation. Intravenous administration may be used but it requires appropriately trained staff to administer, is potentially prone to complications, and is usually the most expensive option. Other routes include transdermal (glyceryl trinitrate patches), rectal (diclofenac, aspirin and carbamazepine suppositories), nebulisation (salbutamol), intramuscular (fosphenytoin) or subcutaneous injections or infusions (opioids, antiemetics and anxiolytic combinations in palliative care). The buccal or sublingual routes may be useful (sublingual lorazepam, nifedipine or buccal glyceryl trinitrate), although they may be unsuitable in mouth injury, impaired mental states, dry mouth or excessive salivation.10 Various preparations such as tablets or hard gelatin capsules have also been given rectally in the palliative care setting.10
Sometimes it may be better to change to a similar preparation which can be given by a different route. For example, buccal prochlorperazine could be used instead of oral metoclopramide, or piroxicam melt instead of an oral non-steroidal anti-inflammatory drug (NSAID). Laxative suppositories such as bisacodyl may be used instead of oral aperients. Dose equivalencies should be considered when changing agents, for example, equivalent doses of fentanyl patches may vary in patients previously on morphine.
Enteral nutrition
When other routes are unsuitable, medication may be administered via enteral feeding tubes in patients on enteral nutrition (EN). Pharmacists need to ensure that systems are in place to identify patients receiving medication through the enteral route, and be proactive in reviewing their medication and providing current literature and guidelines to facilitate drug administration.
Enteral feeding and drug administration may be withheld even in the presence of a feeding tube, particularly after surgery. Patients may be on free drainage or suction as a result of gastrointrestinal dysfunction, or aspirates may be large. In these circumstances it is often assumed that drug absorption would be at best variable, if a drug was absorbed at all. However, some drugs, including angiotensin converting enzyme (ACE) inhibitors and antidepressants are only readily available enterally and, if required, it may be worthwhile to attempt administration of these drugs and closely monitor their effects. The effects may be variable and will alter as the GI tract becomes viable. It may be feasible to suspend drainage or suction, after consultation with medical staff, for long enough to allow the drug to be administered and absorbed. If large aspirates are being produced, drug administration immediately following aspiration may allow the drug to be absorbed.
Prokinetic agents such as cisapride or metoclopramide may be used to encourage restoration of normal gut function and these agents are often prescribed for patients taking enteral feeds. Erythromycin has also been used. Pharmacists should ensure that cisapride is not used in patients with known contraindications to the drug or those who are on drugs which may interact with it, as serious cardiac arrhythmias and cases of sudden death have been reported.11 The manufacturer's data sheet lists the known interactions, but any drug which may inhibit the cytochrome P450 3A4 isoenzyme or prolong the QT interval may also theoretically interact with cisapride.
Drugs and the enteral route Several aspects need to be considered when administering drugs through an enteral feeding tube. Considerations include the practical aspects of administration such as the formulation to be used, whether any interaction with the feed may occur, the type of tube and placement site, and the site of drug absorption.
There is little to be found in the literature on any of these aspects and the manufacturer's summary of product characteristics does not usually include this information. Therefore, most recommendations are theoretical. Usually, drugs are not licensed for use through enteral feeding tubes and pharmacists may need to combine theory with empiricism. Local protocols may help to address specific information needs as well as the unlicensed aspects of drug administration.2
The tubes The tube size and placement site affect drug administration. Fine-bore tubes are unsuitable for some thick liquids and dispersible tablets, for example, omeprazole tablets (which can be dispersed) and cholestyramine sachets.
There are more likely to be problems with absorption when the tube is placed beyond the stomach such as with percutaneous endoscopic jejunostomy (PEJ) tubes. In this case, the pharmacist may place increased importance on the use of alternative routes (eg, suppositories), and should be aware of situations in which the tube may extend beyond the drug's main site of absorption. Drugs that may be affected by this include digoxin, cephalexin, ketoconazole, phenytoin and other anticonvulsants.12 It is necessary for the pharmacist to monitor the patient for signs of a reduction in efficacy of these drugs.
EN: formulations
The preferred and easiest way to administer drugs through a tube is as a liquid preparation. Information on drugs commercially available as a liquid can be found in the British National Formulary (BNF). Additional information on formulations may be found in paediatric formularies and are included in guides produced by the Scottish Neonatal and Paediatric Pharmacists Group and the UK Formulary of Extemporaneous Preparations.13 Sources of information on "specials" include drug manufacturers, manufacturers of suspending agents, local NHS specials units, and specials manufacturers. A list of specials manufacturers has been published.14
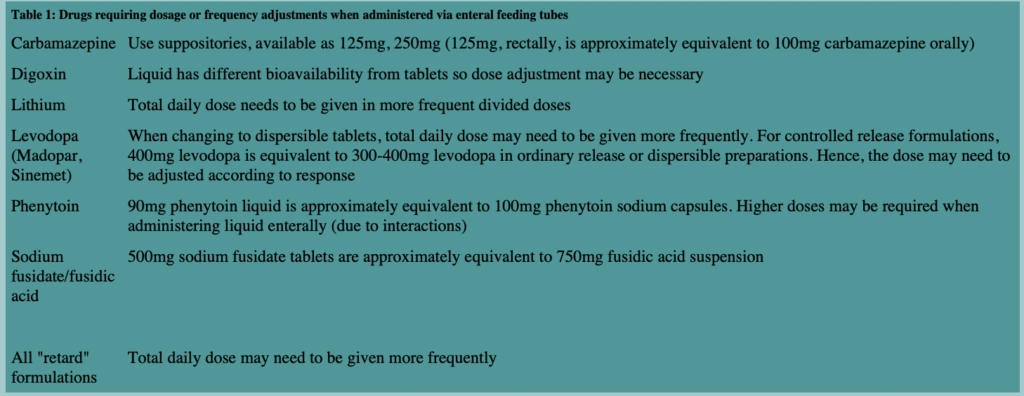
Other formulations that have been administered through a tube are soluble or dispersible tablets, tablets and capsule contents. When changing formulations, drugs may require dosage or frequency adjustments (Table 1).
Liquid preparations Even when a liquid formulation is available, several other factors need to be considered. Not all liquids are suitable for enteral tube administration. Lansoprazole suspension, for example, is too viscous to administer through an enteral tube and sucralfate liquid may be associated with "bezoar" formation. Bezoars are indigestible concretions which may form in the stomach of patients with impaired gastric emptying. Some manufacturers specifically advise dilution of their suspensions before administration through tubes.
Augmentin suspensions should be diluted to half strength to avoid "caking" (personal communication, Smithkline Beecham). Other manufacturers recommend that alternative routes of administration should be used: diazepam liquid is not recommended for enteral tube administration as it is absorbed into the plastic tubing (personal communication, Cox Pharmaceuticals) Conversion to a liquid preparation may involve the use of a different salt which may result in bioavailability changes.
The sorbitol content and osmolality of liquids are associated with GI adverse effects such as sudden-onset osmotic diarrhoea, bloating, stomach cramps,15 and delayed gastric emptying because of the regulatory role of osmoreceptors in the duodenum.16 Excessive use of liquids with a high sorbitol content or osmolality (particularly when patients are on a lot of drugs) should be avoided.
It is important to bear in mind that the symptoms described here could also be related to the enteral feed or infections, such as can be caused by Clostridium difficile.
Many liquids have an osmolality higher than 1000mOsm/kg (compared with the osmolality of GI secretions, which is 100-400 mOsm/kg) but these effects may be avoided by dilution with water (hypotonic), using a formula to calculate volume if necessary,16 or by the use of dispersible tablets. Osmolality may vary, depending on manufacturer and the strength of the preparation. This may or may not be significant, depending on the dose volume employed. For example, digoxin liquid has a high osmolality but in practice this is not problematic because of the low volumes used.12
Cumulative sorbitol doses of 7.5 to 30g may cause adverse effects, with symptoms being particularly severe above 20g. Sorbitol content varies with manufacturer and drug concentration.
The sorbitol content and osmolality of some products have been published elsewhere,17 although these may differ for UK preparations. Most manufacturers' medical information departments can provide information on sorbitol content but osmolality data is often not readily available. However, one USA publication found that only six of 58 commercially available liquids had osmolalities less than, or equal to, 1000mOsm/kg.16 In the absence of data, one approach may be to monitor patients for adverse effects and dilute liquids if necessary, although routine dilution cannot be recommended due to the lack of stability information.
Generally, elixirs or suspensions rather than syrups18 should be used. Syrups with an acidic pH (4 or below) are particularly troublesome as these may "clump" in contact with enteral feeds.19,20
Crushed tablets Lists of tablets which should not be crushed have been published.22,23
Enteric-coated tablets should not be crushed, as the purpose of enteric-coating is to prevent drug dissolution in the stomach and to promote absorption in the small intestine (eg, mesalazine) or to protect the stomach from damage from the drug itself (eg, aspirin).24 If crushed, enteric-coated tablets break into small pieces that clump together when moistened. This results in clogging of the feeding tube.10,17,22
Crushing of slow-release preparations or modified-release preparations destroy their extended release properties and may result in dangerous peaks ("drug dumping") and subtherapeutic troughs, which are of particular concern in drugs with narrow therapeutic indices such as theophylline and lithium.
In some cases, parenteral formulations may be the only suitable or available liquid preparation, but this is usually an expensive option and only suitable for short term use. Excipients such as polyethylene glycol, as found in amiodarone, may preclude the use of this formulation.
Soluble or dispersible tablets If a liquid preparation is unavailable or unsuitable, soluble or dispersible tablets may be an alternative. Tablets not commercially marketed as dispersible may disperse in water. A list of commonly used tablets in the UK which are dispersible has been published.21 This may be a useful and convenient way to administer drugs, avoiding delays in preparing extemporaneous liquids, as well as the problems described above. Specific advice is available from the manufacturers on the dispersion of omeprazole dispersible tablets for use in enteral feeding tubes (personal communication, Astra Zeneca).
Tablets and capsules If all else fails, the possibility of crushing tablets or opening capsules and flushing their contents down the tube could be investigated.
Buccal or sublingual preparations are designed to avoid the GI tract and first pass metabolism. Consequently, the doses tend to be low and therefore insufficient if they are crushed and given through an enteral tube (though administration of these drugs by the buccal or sublingual route may of course be a useful alternative). Chewable tablets and pancreatic enzymes may also not be crushed.
Cytotoxic drugs should not be crushed due to the potential risk to staff from aerosolisation of particles. Local policies should be in place for pharmacy staff preparing cytotoxic suspensions. For example, a formula to prepare azathioprine suspension is available but the manufacturers point out that azathioprine injection is specifically licensed for patients who are unable to swallow tablets. On the other hand, azathioprine tablets readily disperse21 and this may be an acceptable alternative. Generally, cytotoxic tablets, hormone preparations, antibiotics and prostaglandin analogues are not to be crushed. However, some circumstances may require that these preparations be crushed. In these cases, a COSHH (Control of Substances Hazardous to Health) regulations assessment should be carried out to assess the risks to staff handling these drugs.
Some drugs, for example, amiodarone, are not normally crushed and given orally due to their bitter taste. However, they can be crushed for administration through the tube. When crushing light-sensitive drugs such as nimodipine, precautions should be taken to minimise exposure to light. Drugs with a high incidence of allergy (eg, antibiotics) should not normally be crushed due to the risk of cross-contamination from tablet crushing devices.
It is essential that the tablet crushing process is carried out in a safe and effective manner. One way of achieving this is to use a tablet crusher specifically designed for this purpose, or a tablet crushing dispenser which allows staff to crush, disperse and administer the medication in one unit.Tablet crushers are intended for single patient use and should be cleaned with detergent between drug administration and left to air dry, or otherwise handled in line with local policies.
A major safety concern in recent years relates to the inappropriate use of intravenous (IV) syringes for the measurement and administration of drugs intended for oral administration.25,26 Fatalities have resulted when two preparations (phenytoin and potassium chloride), both intended for oral administration, were accidentally given intravenously because they had been drawn up in IV syringes. These cases highlight the need for policies to ensure that such tragedies are not repeated. Drugs intended for administration through enteral tubes should be drawn up and administered using an oral medication syringe. These syringes are now being designed with a wider tip so that they will not fit into hypodermic needles or ports on IV lines. Oral medication syringes are available in a range of sizes, can be used in conjunction with connectors to fit enteral tubes if necessary, and can also be obtained in an amber colour if required for light-sensitive drugs.
Capsule contents Hard gelatin capsules, which often contain a powdered drug, may be pulled open and the contents thoroughly mixed with water before administration. The pellets inside some microencapsulated dosage forms need to be administered intact, and may only be suitable for administration through wide-bore tubes.
The contents of some soft gelatin capsules, for example, choral hydrate and nifedipine, may also be withdrawn and administered through the tube. Nifedipine is light-sensitive and this necessitates rapid administration. This method is not always suitable. For example, doxycycline capsules contain the irritant hydrate form; the contents of some capsules may block the tube; and some capsules contain enteric-coated granules (eg, omeprazole, lansoprazole, itraconazole). Specific advice may be available from the manufacturers or in the literature.27,28,29
EN: drug administration
Once a suitable drug preparation has been identified, the principles in Panel 2 may be used in administering the medication through the feeding tube, although recommendations vary, usually depending on practice or opinion rather than research. Tap water is usually adequate unless chelation with the drug and ions in tap water is known to be a problem, for example, with ciprofloxacin or doxazosin. In these cases, sterile water should be used. The amount of water used should be documented on the appropriate fluid balance sheets. If the patient is fluid-restricted this may be important, particularly where multiple drugs are being given. Alternative routes of administration may be required in such patients.
Panel 2: Techniques for administering drugs via enteral feeding tubes23
1. Crush tablets or open capsules and mix in 10-15ml of tap water (5-10ml for children). Rinse the tablet crusher and flush washings down the tube
2. Dissolve dispersible tablets in 10-15ml of tap water
3. Shake liquid formulations in the bottle
4. Draw up medication into a 50ml needleless oral syringe
5. Flush the nasogastric tube with 30ml of water before drug administration
6. Administer each drug separately, flushing the tube with 5ml of water (3ml for children) in between each medication. Flush the syringe in between medications
7. Flush tube with water after administration is complete
Timing of drug administration Appropriate timing of medication in relation to feeds may help minimise drug-feed interactions, and, as with oral medication, help maximise absorption of drugs such as flucloxacillin, while protecting the GI tract from damage caused by local irritation of the medication (eg, NSAIDs). Ensuring that drug administration times are recorded accurately may help to identify and resolve problems such as those associated with potential interactions.10
Timing will obviously depend on whether the feed is being administered as an intermittent or continuous regimen, and how often drugs need to be administered. Careful consideration may minimise the impact on intake of feed but feed contents or rate of administration may need to be reviewed to compensate for time lost during drug administration. When breaks in feeding are required, a drug may be administered at the lowest frequency possible (eg, phenytoin as a single daily dose), depending on its pharmacokinetics.
For drugs requiring administration on an empty stomach, various recommendations have been made.10,30 It would seem reasonable to stop feeding 30 minutes before drug administration to facilitate gastric emptying and resumed 30 minutes to an hour after, to allow time for drug absorption. These times may need to be extended if gastric motility is poor. This is not required for duodenal or jejunal tubes as feeds are not retained in this part of the intestine.10
Addition of drugs to enteral feeds Although there are theoretical reasons why administration directly to the feed would be of benefit, including the avoidance of gastrointestinal intolerance associated with bolus administration of some medicines through a feeding tube, adding drugs to the enteral feed is generally discouraged for the following reasons:
- lack of information on potential interactions which may occur
- the possibility of microbial contamination
- an increased risk of tube blockage due to coagulation of feed proteins, or "clumping" of the feed formulation which can also alter drug stability
This technique has been used in some specific circumstances. In the USA, oral morphine sulphate has been added to specific enteral formulations in some palliative care settings to try to ease the technical burden of administration on carers.31,32 Addition of ranitidine to enteral feeds has been suggested to improve maintenance of pH above 4 for stress ulcer prophylaxis.33 These practices cannot, however, be recommended without further research into bioavailability and compatibility with specific UK feed formulations.
Tube blockage Occlusion of small-bore feeding tubes may occur in up to 15 per cent of patients and occupies nursing time, limits patients' feed and drug intake, and increases trauma to the patient. The trauma would be compounded if additional surgical intervention was required to replace percutaneous endoscopic gastrostomy (PEG) and PEJ tubes and is also associated with increased costs.34,6
Blockage may also result in tearing of the tube, causing direct administration of enteral feeds to the oesophagus. This is also associated with the formation of oesophageal bezoars.35,36,37 In particular, sucralfate's properties of forming an insoluble gelatinous substance in the presence of acid, as well as its tendency to delay gastric motility, predisposes it to the formation of bezoars. Sucralfate may also bind with antacids and proteins in enteral feeds. Sucralfate has caused both oesophageal bezoar formation and blockage of nasogastric tubes in patients being enterally fed. Hence, it is recommended that feeding be stopped one hour before and one hour after each dose of sucralfate. This leads to the loss of 12 hours feeding if used at the recommended dose for stress ulcer prophylaxis (personal communication, Chugai Pharma).
The likelihood of obstruction may increase with the number of medicines administered but is often associated with coagulation of the feed formula rather than mechanical blockage of the tube by medicines.
Other related factors include feed formulation (high protein content, use of intact casein molecules as the protein source, high viscosity, low pH), rate of administration (intermittent versus continuous),38 and feeding tube design.39
Bulk-forming drugs may block tubes and may be avoided by using an enteral feed with a fibre content instead. Tubes delivering to the stomach where the contents are at a low pH have shown higher occlusion rates than those delivering further down the GI tract where the pH is higher. Factors which may contribute to lower rates of obstruction include pharmacist advice, nurse training and avoidance of inappropriate tablet crushing.6,40 Tube blockage may be avoided by:
- using appropriate formulations
- ensuring tablets are fully crushed, if appropriate
- using correct flushing techniques
- avoiding drug interactions with feeds (see below)
- avoiding the use of acidic liquids
- consideration of feeding tube size (small-bore tubes are more likely to clog)
Addition of additives such as docusate sodium and simethicone emulsion to feeds to prevent clogging has shown no advantage.38 Prophylactic locking of tubes with alkalinised pancreatic enzymes may be associated with decreased tube occlusion41 but there is insufficient evidence to bring this into routine practice.
Various anecdotal approaches have been used to clear blocked tubes (Panel 3) but there is no substantial evidence that any of these are more effective than plain water. The usefulness of pancreatic enzymes may depend on the pH at which they are administered.42 Acidic agents such as cranberry juice or carbonated drinks may even exacerbate the problem by causing feed coagulation.
Panel 3: Unclogging enteral feeding tubes
The following have been used for unclogging enteral feeding tubes:34,42,70,71,72
- Cranberry juice
- Carbonated drinks
- Warm water
- Meat tenderiser (contains papain, a mixture of proteolytic enzymes)
- Pancreatic enzymes (alkalinised solution)
- Clog Zapper (a commercially available food grade powder designed to break up formula clogs in most enteral feeding devices)
NB: There is no substantial evidence in the literature for most of these
EN: interactions
Drugs may interact directly or indirectly with enteral feeds. Some of the more common examples are discussed below, but some of the factors which may prompt pharmacists to check for possible interactions include:
- drugs which interact with food, vitamins or electrolytes, or need to be given on an empty stomach
- drugs which are given in liquid form (check acidity, osmolality, sorbitol content), particularly when multiple drugs or high volumes are given this way
- drugs with a narrow therapeutic index
Consideration should be given to appropriate monitoring for altered response or altered plasma levels (phenytoin, theophylline, etc). If drug interactions are not identified but doses are adjusted due to lack of therapeutic response, toxicity may ensue when feeds are discontinued, particularly in drugs with a narrow therapeutic index.
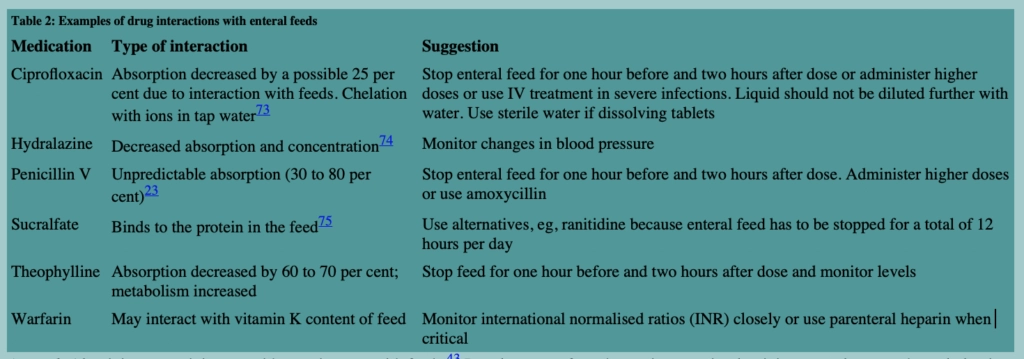
The management of drug interactions with feeds may depend on whether the feed is being administered continually or as intermittent boluses (see "Timing of drug administration", above). The compatibility of some drugs (fluconazole, cephalexin, diazepam, propranolol, morphine, ranitidine) with feeds has been described but this may depend on feed formulation.10 Possible interactions which may cause precipitation of enteral feeds such as that between acidic liquids and enteric-coated granules inside capsules have already been discussed. Some of the more common drugs which may interact with enteral feeds are described below (see also Table 2).
Antacids Aluminium-containing antacids may interact with feeds.43 Development of an obstructing protein-aluminium complex oesophageal plug in patients given aluminium/magnesium hydroxide while receiving high protein enteral feeds has been described.44 It has been suggested that antacids should not be given to patients receiving these high molecular weight protein feeds or, if necessary, the feed should be stopped and the tube thoroughly flushed. Antacids may also bind phosphate from enteral feeds, thereby causing hypophosphataemia.
Anticonvulsants Many patients on anticonvulsant therapy are also enterally fed. Phenytoin and carbamazepine are two of the anticonvulsants commonly employed.
Phenytoin The effects of enteral feeds on phenytoin can be further complicated by the presence of interacting drugs (especially in patients on multiple anticonvulsant therapy), and the altered distribution of phenytoin in patients with low albumin. Phenytoin suspension given undiluted and without flushing may result in 75 per cent of the initial dose being retained in the tubing. The liquid is viscous and must be properly shaken before each administration to avoid variations in dosing. A reduction in the absorption of phenytoin may result from a combination of physicochemical factors including:
- binding to the feeding tube (or to proteins or electrolytes in feeds)
- inadequate dissolution due to the high pKa of phenytoin and the acidic nature of enteral formulae
- decreased transit time due to hyperosmolar feeds or enteral feed-associated diarrhoea
The phenytoin interaction is well documented and may cause significant problems in attaining and maintaining therapeutic levels of phenytoin in clinical practice, even when the various recommendations45,46,47 to minimise the interaction are followed (see Panel 4). In some cases parenteral therapy may be required, for example with intramuscular fosphenytoin. A recent study of the use of phenytoin sodium powder from capsules, instead of the acid salt in the liquid, found no evidence of improved absorption.48
Panel 4: Minimising interactions between liquid phenytoin and enteral feeds
1. Give phenytoin as a single daily dose
2. Stop enteral feed two hours before administration of phenytoin and recommence two hours after dosing
or
Suspend feed between 10pm and 6am (that is, during sleeping hours) and give phenytoin as a single daily dose at midnight (this allows for six hours drug absorption)
3. Dilute phenytoin suspension with at least equal parts (dilution up to 1:3 has also been recommended) or at least 20ml water (remember to shake the bottle before use)
4. Flush enteral tube with plenty of water before and after administration
When phenytoin capsules are substituted for phenytoin liquid, serum level monitoring is advised and dose should be adjusted accordingly. The dosage form and volume of liquid should always be documented on the patient's prescription chart to avoid confusion
Carbamazepine Carbamazepine suppositories are specifically licensed for administration as short term replacement therapy for patients in whom oral replacement therapy is not possible. Carbamazepine liquid may however be considered, particularly in patients with long term lack of oral access with feeding tube in situ and several studies have assessed this method.49,50,51 Conflicting evidence for reduced bioavailability with enteral feeds may reflect differences in feed content. Carbamazepine may also adhere to the tube itself, although it has recently been reformulated as a less viscous liquid which may reduce this problem. Absorption may also be impaired where tubes are placed beyond the stomach. Suggested management options include dilution of liquid with sterile water or normal saline solution, separation of feed and drug administration times and close monitoring of plasma carbamazepine levels. It may however be that co-administration of enteral feeds has a beneficial effect in reducing toxicity associated with high peak levels attained after rapid absorption of carbamazepine liquid.52 Stopping enteral feeds may be considered where rapid attainment of therapeutic levels are required.53
Other anticonvulsants Phenobarbitone, valproate, gabapentin, topiramate, lamotrigine and vigabatrin are not thought to interact with enteral feeds .
Warfarin The interaction between oral anticoagulants and enteral feeds is well documented.54,55 The vitamin K content of feeds may antagonise warfarin's effect on the synthesis of clotting factors, resulting in a reduced therapeutic effect. Effects on plasma protein binding of warfarin and enteral feeds in the gut may also contribute. A three-hour gap between stopping the feed and administering warfarin has been used to minimise this effect but there is insufficient evidence to recommend this routinely. Patients prescribed warfarin should be monitored carefully when fed in this way and the anticoagulant dose increased as necessary. The dose of warfarin while on enteral feeds may differ from that used when the patient is on a normal oral diet. Therefore, it is essential to review dose requirements once feeds are discontinued. The interaction between warfarin and vitamin K in feeds has been reported with various enteral feeds (although some manufacturers have reformulated feeds to avoid this problem). Pharmacists may find it useful to be aware of the vitamin K content of feeds used locally. (NB: A normal daily diet in the western world contains 300 to 500mcg of vitamin K). As little as 50mcg of vitamin K may cause a change in prothrombin time.2
Theophylline The bioavailability of theophylline may be altered by food in general, and differences in pharmacokinetics may be related to the protein and carbohydrate contents of diet.54 The mechanism may be related to changes in metabolism as a result of protein and carbohydrate effects on stimulating and inhibiting cytochrome P450. Varying effects have been reported in patients on enteral feeds. Both decreased and increased absorption have been reported. It may be advisable to stop feeds before and after administration and to monitor plasma levels of the drug.
Quinolone antibiotics Quinolone antibiotics such as ciprofloxacin and ofloxacin possess good absorption characteristics, so they are usually given enterally rather than intravenously. When they are given intravenously, an early stepdown to the oral route is normally recommended. However, in patients receiving enteral feeding, studies suggest that significantly lower plasma concentrations than expected are attained.56,57 The mechanism for this interaction is the formation of insoluble chelates with divalent ions (calcium, magnesium, etc) in the feeds, thus reducing absorption from the GI tract.
Where a severe infection is being treated it has been suggested that NG tube administration to these patients should not be used unless facilities for plasma concentration monitoring are available.56 In other patients, consideration may be given to prescribing larger doses to be given through the enteral feeding tube.2
Although ofloxacin is considered to exhibit this phenomenon to a lesser extent, the interaction is thought to be a class effect and should be managed accordingly.57
Total parenteral nutrition
Total parenteral nutrition, or TPN, is employed in patients where an adequate dietary intake cannot be maintained via the GI tract. Although many patients will be truly "nil by mouth", some may still be able to receive and absorb medicines given orally and in such cases this remains the preferred route.
If alternative routes are unsuitable, parenteral administration of drugs may be required. Where possible, these should be given separately from the TPN solution but this is not always possible, particularly in areas where the number of IV drugs required exceeds the access sites available such as in cancer and intensive care unit (ICU) patients. In these cases, there may be no alternative but to administer the drug simultaneously with the TPN fluid.
TPN: incompatibilities
Although intravenous drug-drug incompatibilities have been described elsewhere,58 less is known about drug-parenteral feed incompatibilities. This is due partly to the huge variability in composition of TPN solutions, and the range and concentration of drugs which may be administered simultaneously. In addition, many of the reports in the literature relate only to physical stability and have not addressed the potential for chemical instability.
Factors which affect drug and TPN stability and compatibility include:
- composition of TPN regimen
- contact time between drug and TPN solution:
- brand and concentration of drug added
- exposure of admixture to temperature and light
Other issues to be considered when the TPN is a 3-in-1 admixture containing a fat emulsion include the stability of the emulsion, the bioavailability of drug from emulsion and the formation of precipitates which may be obscured by the fat emulsion itself. Intralipid is an example of a fat emulsion commonly used.
TPN: drug administration
The extent to which the factors described above affect the stability and compatibility of TPN may be influenced by the way in which the parenteral feed and drugs are administered.
The multi-lumen catheter Where TPN is administered via a multi-lumen catheter, any drug administered through a different lumen will enter the bloodstream at a different point and is usually regarded as being administered by a separate line. Such administration ensures minimal contact time between the drug and TPN solution and hence reduces the risk of incompatibility. Incompatibilities are therefore restricted to drugs passing through the same lumen. Hence, single-lumen, peripherally-inserted central catheters, which may be used for TPN administration, may be less suitable for concomitant drug administration.
Although an in vitro study of simultaneous phenytoin and TPN infusion in multi-lumen catheters observed phenytoin precipitation near the tip of a double lumen but not a triple lumen catheter,59 it appears to be an isolated report.
Y-site connection Y-site connection should only become a necessity when there is no other route or parenteral access available and when a multi-lumen catheter is being used to full capacity. Ideally, the lumen intended for administration of TPN should be "protected" from the addition of further drugs, but this may not be possible in intensive care units.
Y-site delivery often allows administration of drugs that cannot be given together in the same solution and examples of this have been cited.58 There is, however, little information on the compatibility of drugs during Y-site administration with TPN solutions. Although the compatibility of some drugs have been tested and reported with TPN solutions,60,61 these reports cite specific TPN solutions, drug concentrations and contact times and cannot be extrapolated to different drug concentrations or longer contact times. The contact time between two or more solutions administered through a Y-site tends to be short, often in the range of 15 to 30 minutes and generally not more than 60 minutes.58
It has been suggested that relatively few drug combinations are so chemically unstable that they could not be given via a Y-site and that as long as they are physically compatible they can often be administered in this way.58,61 However, a report evaluated the physical compatibility of 106 drugs during simulated Y-site injection into nine different parenteral nutrition admixtures and found 23 drugs (including aciclovir, dopamine, ondansetron) to be incompatible with the TPN solution.60
Addition of drugs to parenteral feeds This practice is not recommended and should be actively discouraged in the absence of stability or compatibility data relating to specific TPN regimens and drug concentrations.
There is a significant potential for drug stability and compatibility problems when drugs are added to TPN solutions, not least as a result of the prolonged duration of contact time and exposure to temperature and light. In addition, TPN solutions are composed of numerous constituents with the potential to interact with drug additives. With 3-in-1 admixtures, the potential for incompatibility and stability problems is increased due to the addition of a fat emulsion. It has been recommended that no other drugs or solutions be added to fat solutions due to the risk of disturbing the stability of the emulsion or affecting the bioavailability of the drug.58
A significant risk is that of a precipitate forming but being obscured by the fat emulsion. Unrecognised calcium phosphate precipitation in a 3-in-1 parenteral nutrition mixture resulted in the death of a patient.62 Drug additions to TPN solutions should therefore never be undertaken unless sufficient data exists to ensure stability of the final product. Companies involved in the production of TPN components often have stability data on the addition of a range of drugs to their particular product and provide a useful source of information and advice when required.
Ranitidine is one example of a drug that is sometimes added to TPN (both with and without lipid) on the basis of stability data with specific formulations.63,64
In conclusion, where no other option exists but to administer drugs through the same access site as TPN, it is best to use a separate lumen in a multi-lumen catheter in order to avoid the potential for drug-parenteral feed incompatibilities. Additional peripheral access may be sought, if necessary, and administration of the drug via a Y-site connection can be considered. Addition of any drug to a TPN solution should only be used as a last resort.
TPN: interactions
Drug interactions with TPN solutions are not reported in the literature as commonly as those relating to drug interactions with enteral feeding solutions. Some examples of reported interactions are described below. In addition to these specific examples, general issues such as drug-induced effects on electrolytes and cumulative fluid volumes should also be considered.
Warfarin Warfarin resistance was noted in a patient receiving a TPN solution containing Intralipid. Discontinuation of this infusion and re-challenging the patient with warfarin resulted in an increase in his prothrombin time.54,65 A similar response to warfarin was seen in a second patient who received propofol infusion, resulting in a reversal of the effects of both enteral and intravenous warfarin.8 Propofol (Diprivan) contains soybean oil 10 per cent and has a fatty acid profile similar to that of Intralipid. Both preparations contain similar amounts of vitamin K. A review of the literature suggested possible ways in which the activity of warfarin could be affected by lipid emulsions.8 Lipid emulsions may increase the production of clotting factors, supply sufficient vitamin K to antagonise the effect of warfarin or facilitate platelet aggregation. They may also facilitate warfarin binding to albumin, resulting in a reduction in the level of free unbound drug and a subsequent reduction in activity.
In practice, pharmacists may consider the possibility of interactions when otherwise unexplained changes in anticoagulant activity are seen in patients on TPN and warfarin. Large doses of warfarin may be required and INRs should be checked regularly to ensure adequate anticoagulation.
Theophylline One case report of an elderly woman treated with IV aminophylline described a marked fall in theophylline levels when the amino acid concentration of her TPN solution was increased.66 A study in seven patients with malnutrition, however, found only small, probably insignificant changes in theophylline pharmacokinetics while on TPN.53,67
Phenytoin A single case report of a 40-year old man described decreased total phenytoin levels during the administration of TPN, which subsequently increased to pre-TPN levels following discontinuation of TPN. The authors suggested that this may be due to increased protein intake from TPN, resulting in increased microsomal oxidative metabolism and hence reduced plasma levels.
Free phenytoin levels were not, however, measured and so this factor could not be addressed.68
Propofol Propofol, which is formulated as a lipid emulsion similar to Intralipid 10 per cent, is included in sedation policies of many ICU areas and is occasionally administered to patients receiving fat-containing TPN. However, accumulation of fat may occur within the circulation if lipoprotein lipase becomes saturated and if fat is infused faster than it can be eliminated. The amount of lipid emulsion infused may be significant, especially in critically ill patients who may have impaired fat metabolism.69 Close monitoring of serum triglyceride concentrations and reduction in fat administration, if required, is recommended in such patients to avoid "fat overload" (personal communication, Astra Zeneca).
Conclusion
As previously stated, the majority of the information on drug administration via enteral feeding tubes cannot be supported except by anecdotal experiences, practical or theoretical considerations, or very limited anecdotal evidence in the literature. In most cases, no published data exists to confirm the safety of these suggestions, and most drugs are not licensed for administration in this way. Local pharmacy departments may wish to develop written policies to address these issues.
There are many drug delivery issues to be considered in patients receiving enteral or parenteral nutritrion. The pharmacist is in a unique position to advise and liaise with the multi-disciplinary team and with patients and carers to ensure optimum drug delivery in these patients.
Acknowledgments: We would like to thank our local drug information, sterile products and nutrition team colleagues, and manufacturers' medical information departments who have assisted in providing us with information for this article, and the drug information pharmacists in the UK network for their interest in, and comments on, our local guidelines.
References
| 1. Allison SP. Malnutrition in hospital patients. Hospital Update 1995;2:55-62. |
| 2. Smith A. Inside story. Nurs Times 1997;93:65-9. |
| 3. Mason P. Diet and drug interactions. Pharm J 1995;255:94-7. |
| 4. Cerulli J, Malone M. Assessment of drug-related problems in clinical nutrition patients. JPEN 1999;23:218-21. |
| 5. Naysmith MR, Nicholson J. Nasogastric drug administration. Prof Nurse 1998;13:424-7. |
| 6. Belknap DC, Seifert CF, Petermann M. Administration of medications through enteral feeding catheters. Am J Crit Care 1997;6:382-92. |
| 7. Dykes RG. A pharmaceutical needs assessment of patients in the community with enteral feeding tubes [MSc thesis]. Derby:University of Derby;1999. |
| 8. McLaren R, Washman BA, Swift DK, Kuhl DA. Warfarin resistance associated with intravenous lipid administration: discussion of propofol and review of the literature. Pharmacotherapy 1997;17:1331-7. |
| 9. Anonymous. Drugs in the peri-operative period: 1. Stopping or continuing drugs around surgery. Drug Ther Bull 1999;37:62-4. |
| 10. Gilbar PJ. A guide to drug administration in palliative care (review). J Pain Symptom Manage 1999;17:197-207. |
| 11. Cisapride (Prepulsid): Risk of arrhythmias. Committee on Safety of Medicines. Current problems in pharmacovigilance. 1998; 24:1. |
| 12. Adams D. Administration of drugs through a jejunostomy tube. Br J Int Care 1994;4:10-7. |
| 13. Grassby, PF, editor. UK formulary of extemporaneous preparations. Penarth:1995. |
| 14. Thompson M. Specials manufacturing. Who makes specials and why? Pharm J 1995;254:226-31. |
| 15. Holtz L, Milton J, Sturek JK. Compatibility of medications with enteral feedings. JPEN 1987;11:183-6. |
| 16. Estoup M. Approaches and limitations of medication delivery in patients with enteral feeding tubes. Critical Care Nurse 1994;14:68-72,77-9. |
| 17. Beckwith MC, Barton RG, Graves CA. Guide to drug therapy in patients with enteral feeding tubes: dosage form selection and administration methods. Hosp Pharm 1997;32:57-64. |
| 18. Williams PJ. How do you keep medicines from clogging feeding tubes? Am J Nursing 1989;7:181-2. |
| 20. Cutie AJ, Altman E, Lenkel L. Compatibility of enteral products with commonly employed drug additives. JPEN 1983;7:186-91. |
| 21. Mistry B, Samuel L, Bowden S, McArtney RJ, Roberts DE. Simplifying drug therapy for patients with swallowing difficulties. Pharm J 1995;254:808-9. |
| 22. Mitchell JF. Oral dosage forms that should not be crushed:1998 update. Hosp Pharm 1998;33:399-415. |
| 23. Engle KK, Hannawa TE. Techniques for administering oral medications to critical care patients receiving continuous enteral nutrition. Am J Health-Syst Pharm 1999;56:1441-4. |
| 24. Woolfrey S, Geddes A, Hussain A, Cox J. Percutaneous endoscopic gastrostomy. Pharm J 1996;257:181-4. |
| 25. Cousins DH, Upton DR. Medication errors. Pharm in Pract 1997;7:597-8. |
| 26. Cousins DH, Upton DR. Medication errors. Pharmacy in Practice 1998;8:209-10. |
| 27. Ong DL, Fobes LM. Administering itraconazole via nasogastric tube. Am J Health-Syst Pharm 1996;53:1962. |
| 28. McAndrews KL, Eastham JH. Omeprazole and lansoprazole suspensions for nasogastric administration. Am J Health-Syst Pharm 1999;56:81. |
| 29. Peckman HJ. Alternative method for administering proton pump inhibitors through nasogastric tubes. Am J Health-Syst Pharm 1999;56:1020. |
| 30. Miller D, Miller H. Giving medicines through the tube. Registered Nurse 1995;58:44-7. |
| 31. Michelini TJ, Bhargaya VO, Dube JE. Stability of oral morphine sulphate solution in two enteral tube feeding products. Am J Hosp Pharm 1988;45:628-30. |
| 32. Udeani GO, Bass J, Johnston TP. Compatibility of oral morphine sulphate solution with enteral feeding products. Ann Pharmacother 1994;28:451-5. |
| 33. Crowther RS, Bellanger R, Szauter KEM. In vitro stability of ranitidine hydrochloride in enteral nutrient formulas. Ann Pharmacother 1995;29:859-62. |
| 34. Marcuard SP, Perkins AN. Clogging of feeding tubes. JPEN 1988;12:403-5. |
| 35. Cremer AS, Gelfand DW. Oesophageal bezoar resulting from enteral feedings. JPEN 1996;20:371-3. |
| 36. Garcia-Luna PP. Oesophageal obstruction by solidification of the enteral feed: a complication to be prevented. Intensive Care Med 1997;23:790-2. |
| 37. Irgau I, Fulda GJ. Oesophageal obstruction secondary to concretions of tube-feeding formula. Crit Care Med 1995;23:208-10. |
| 38. Hofstetter J, Allen LV Jr. Causes of non-medication-induced nasogastric tube occlusion. Am J Hosp Pharm 1992;49:603-7. |
| 39. Benson DW, Griggs BA, Hamilton F, Hiyama DT, Bower RH. Clogging of feeding tubes: a randomised trial of a newly designed tube. Nutr Clin Pract 1990;5:107-10. |
| 40. Seifert CF, Frye JL, Belknap DC, Anderson DC. A nursing survey to determine the characteristics of medication administration through enteral feeding catheters. Clin Nurs Res 1995;4:290-305. |
| 41. Sriram K, Jayanth V, Lakshmi RG, George VS. Prophylactic locking of enteral feeding tubes with pancreatic enzymes. JPEN 1997;21:353-6. |
| 42. Marcuard SP, Stegall KL, Trogdon S. Clearing obstructed feeding tubes. JPEN 1989;13:81-3. |
| 43. Tomlin ME, Dixon S. Aluminium and nasogastric feeds [letter]. PharmJ 1996;256:40. |
| 44. Valli C, Schulthess H-K, Asper R, Escher F, Hacki W. Interaction of nutrients with antacids: a complication during enteral tube feeding. Lancet 1986;i(8483):747-8. |
| 45. Fleischer D, Sheth N, Kou JH. Phenytoin interaction with enteral feedings administered through nasogastric tubes. JPEN 1990;14:513-6. |
| 46. Krueger KA. Effect of two administration schedules of an enteral nutrient formula on phenytoin bioavailability. Epilepsia 1987;28:706-12. |
| 47. Rodman DP, Stevenson TL, Ray TR. Phenytoin malabsorption after jejunostomy tube delivery. Pharmacotherapy 1995;15:801-5. |
| 48. Doak KK, Haas CE, Dunnigan KJ, Reiss RA, Reiser JR, Huntress J et al. Bioavailability of phenytoin acid and phenytoin sodium with enteral feedings. Pharmacotherapy 1998;18:637-45. |
| 49. Kassam RM, Friesen E, Locock RA. In vitro recovery of carbamazepine from Ensure. JPEN 1989;13:272-6. |
| 50. Randall C, Tett S, Lauchlan R. Effect of enteral feeds on anticonvulsant concentrations. Clin Exp Pharmacol Physiol 1991;suppl 18:50. |
| 51. Clark-Schmidt AL, Garnett WR, Lowe DR, Karnes HT. Loss of carbamazepine suspension through nasogastric feeding tubes. Am J Hosp Pharm 1990; 47:2034-7. |
| 52. Bass J, Miles MV, Tennison MB, Holcombe BJ, Thorn MD. Effects of enteral tube feeding on the absorption and pharmacokinetic profile of carbamazepine suspension. Epilepsia 1989;30:364-369. |
| 53. Miles MV, Lawless ST, Tennison MB, Zaritsky AL, Greenwood RS. Rapid loading of critically ill patients with carbamazepine suspension. Paediatrics 1990;86:263-66. |
| 54. Stockley IH. Drug interactions. 4th ed. London:The Pharmaceutical Press;1996. |
| 55. Martin JE, Lutomski DM. Warfarin resistance and enteral feedings. JPEN 1989;13(2):206-8. |
| 56. Mimoz O, Binter V, Jacolot A, Edouard A, Tod M, Petitjean O et al. Pharmaco-kinetics and absolute bioavailability of ciprofloxacin administered through a nasogastric tube with continuous enteral feeding to critically ill patients. Intensive Care Med 1998;24:1047-51. |
| 57. Mueller BA, Brierton DG, Abel SR, Bowman L. Effect of enteral feeding with Ensure on oral bioavailabilities of ofloxacin and ciprofloxacin. Antimicrob Agents Chemother 1994;38:2101-5. |
| 58. Trissel LA. Handbook on injectable drugs. Maryland:American Society of Health-System Pharmacists;1998. |
| 59. Collins JL, Lutz RJ. In vitro study of simultaneous infusion of incompatible drugs in multi-lumen catheters. Heart Lung 1991;20:271-7. |
| 60. Trissel LA, Gilbert DL, Martinez JF, Baker MB, Walter WV, Mirtallo JM. Compatibility of medications with 3-in-1 parenteral nutrition admixtures. JPEN 1999;23:67-74. |
| 61. Trissel LA, Gilbert DL, Martinez JF, Baker MB, Walter WV, Mirtallo JM. Compatibility of parenteral nutrient solutions with selected drugs during simulated Y-site administration. Am J Health-Syst Pharm 1997;54:1295-300. |
| 62. Hill SE, Heldman LS, Goo EDH, Whippo PE, Perkinson JC. Fatal microvascular pulmonary emboli from precipitation of a total nutrient admixture solution. JPEN 1996;20:81-7. |
| 63. Pearson VE, King LM. An analysis of potential and real cost savings by the addition of ranitidine to total parenteral nutrition solutions. Hosp Pharm 1992;27:610-3. |
| 64. Williams MF, Hak LJ, Dukes G. In vitro evaluation of the stability of ranitidine hydrochloride in total parenteral nutrient mixtures. Am J Health-Syst Pharm 1990;47:1574-9. |
| 65. Lutomski DM, Palascak JE, Bower RH. Warfarin resistance associated with intravenous lipid administration. JPEN 1987;11:316-8. |
| 66. Ziegenbein RC. Theophylline clearance increase from increased amino-acid in a CPN regimen [letter]. DICP 1987;21:220-1. |
| 67. Cuddy PG, Bealer JF, Lyman EL, Pemberton LB. Theophylline disposition following parenteral feeding of malnourished patients. Ann Pharmacotherapy 1993;27:846-51. |
| 68. Messahel FM, Solis GL, Aguwa CN. Does total parenteral nutrition lower serum phenytoin levels? Cur Ther Research 1990;47:1017-20. |
| 69. Van Brandt N, Hantson P, Horsmans Y, Mahieu P, Verbeeck RK. Effect of enteral versus parenteral feeding on hepatic blood flow and steady state propofol pharmacokinetics in ICU patients. Intensive Care Med 1998;24:795-800. |
| 70. Bockus S. Troubleshooting your tube feedings. Am J Nurs 1991;91:24-8. |
| 71. Krupp KB, Heximer B. Going with the flow. How to prevent feeding tubes from clogging. Nursing 1998;28:54-5. |
| 72. Marcuard SP, Stegall KS. Unclogging feeding tubes with pancreatic enzyme. JPEN 1990;14:198-200. |
| 73. Dorrian I. Cost-effectiveness – is it always effective? J Antimicrob Chemother 1997;39:286-8. |
| 74. Semple HA. Interactions between hydralazine and oral nutrients in humans. Ther Drug Monit 1991;13:304-8. |
| 75. Rowbottom SJ, Wilson J, Samuel L, Grant IS. Total oesophageal obstruction in association with combined oral feed and sucralfate therapy. Anaesth Intensive Care 1993;21:372-4. |
Source: https://pharmaceutical-journal.com/article/ld/managing-drug-therapy-in-patients-receiving-enteral-and-parenteral-nutrition
0 Response to "Digoxin and Ferusemide in Enteral Feeding"
Publicar un comentario